Every week, our care navigators sit on video calls with people who are considering psilocybin for the first time. These are not impulsive decisions. Most of the people who reach us have been reading and researching for one to three years before they ever book a call. Many name Michael Pollan, or a story from a friend who went before them. By the time we meet them, they have usually tried a great deal already, and they arrive carrying something heavy.
This post is about the very human, very specific reasons people come to us. It’s also about what the evidence says actually happens to these people in psilocybin journeys. It’s a collection of individual stories and real world findings pulled from thousands of journeys. They tell the same story from two different distances.
Who comes, and why
What strikes us most is how different the reasons are.
- Some come carrying grief that has nowhere to go. One woman lost her husband and her mother within the same few months. A father told us about the child he lost in a car accident. Grief like this often arrives frozen. People describe not being able to fully cry, not being able to feel the thing they know is there. We have written before about psilocybin and the journey through grief, because it comes up so often.
- Some come after years of depression that has not responded to anything. Treatment-resistant depression is the single most common thread we hear. Someone who had cycled through multiple SSRIs and SNRIs arrived emotionally numb, the side effect having become its own problem. Someone who had been in therapy twice a week for years still felt stuck. One person told us that they do not remember being happy, even as a small child. For many of these people, psilocybin is the last thing on a long list, and also the most hopeful. If that is where you are, our explainer on how psilocybin works to treat depression is a good place to start.
- A growing number come to us after ketamine. They tried ketamine or esketamine and found that it either did not work for them or left them disoriented, with no one to help them make sense of what came up. One person booked a call with us the same day as a difficult, unguided ketamine session. What they are looking for, more than a different molecule, is a guided container.
- Some are at the edges of life. A man approaching the end of his asked for help meeting that transition consciously, rather than with fear. Two of our recent callers were adult children reaching out on behalf of a parent: one with early dementia, another for a parent who had been hesitant about psychedelics for years, was finally ready, and wanted their child beside them for it.
- And some come for reasons that have nothing to do with a diagnosis at all. Burnout and career transition show up regularly. One person left a career for a deliberate sabbatical of inner work. A lifelong athlete wanted help with performance anxiety that had shadowed her whole career. Founders come to work on identity, courage, and clarity, which is a personal use case I have written about at length.
The pattern underneath the stories
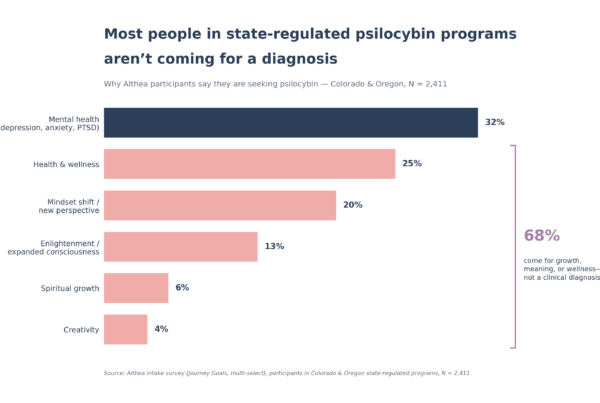
Across more than 4,000 participants in Colorado and Oregon’s regulated programs, only about a third are coming for a clinical mental health condition like depression, anxiety, or PTSD. Roughly two-thirds are coming for something a prescription will never quite name: grief, meaning, creativity, spiritual growth, identity, a way back to feeling.
FDA approvals are advancing, and they will be narrowly indicated, written for specific diagnoses. Those labels could eventually reach perhaps a third of the people we already see. The other two-thirds will still be looking for somewhere legal and supported to go. The reasons people seek this work are far wider than any label, and they are not going away.
It is worth saying that the line between clinical and not clinical is softer than it sounds. Many of the people who come to us for growth or grief also carry long histories of depression, anxiety, or trauma. The reason someone gives for booking a call is rarely the same as the sum of what they are carrying.
What happens to them
So what actually changes?
This is where the individual stories meet the data. We can answer the question at scale because the outcome measures are built into the Althea platform that facilitators already use to document their work. Analyzing thousands of experiences, the short version is that people get better, and the size of the change is large.
Among participants with paired before-and-after data, depression scores (PHQ-9) fell by about half, and just over half of those participants dropped below the clinical threshold entirely. Anxiety scores (GAD-7) fell by a similar amount, with most participants seeing at least a fifty percent improvement. The effect sizes are large and comparable to what controlled clinical trials have reported. Improvement did not depend on how sick someone was to begin with. People who started with mild symptoms and people who started with severe symptoms improved comparably.
That last point speaks directly to the two-thirds who do not arrive with a diagnosis. Even among participants who were not clinically depressed or anxious, well-being scores rose (WHO-5). For the people who started with the lowest well-being, the change was dramatic, with scores more than doubling. The benefit is not confined to the most acute cases. It shows up across the same range of reasons people walk in with.
For the large group who arrive already on antidepressants, there is a practical finding worth knowing. Participants taking SSRIs or SNRIs saw equivalent benefit, with no need to taper off first. That removes a barrier that has historically kept many people from even trying.
We are careful about what we claim. This is a two-week window, not a long-term followup, and our observations carry the limitations any early real-world evidence does: it is observational rather than a controlled trial, the follow-up is short, and the population is not yet as diverse as it needs to be. What it offers that a controlled trial cannot is ecological validity at scale: thousands of real people, with real comorbidities, in real settings, making real decisions about their own care.
The throughline
Here is the contrast: The reasons people come are almost infinitely specific. A widow. A father. A burned-out executive. A physician who went numb. A parent calling for a parent. The impact, when it comes, shows up across all of them.
That is the thing the anecdotes and the data agree on from their two different distances. Whether someone arrives with a diagnosis or with a question they cannot quite put into words, the full protocol tends to move them. Not the medicine alone, but the medicine together with a facilitator, real preparation, and the integration work afterward. And because this happens inside the regulated programs, the facilitators are licensed, the cultivation is regulated, and the experience is supervised, which is what separates it from the underground entirely.
Whatever brings you, there is a structured, legal way to do this work, and resources to help you understand it before you decide. We have written about psilocybin for depression, anxiety, PTSD, anorexia, grief, and for founders working on themselves. If you find yourself somewhere on that spectrum, or somewhere it does not quite name, that is exactly who this is for.
When you are ready, you can browse experiences and find a facilitator who fits what you are carrying. Or if you’d like to talk it through with one of our psychedelic care navigators, you book a call here.